Report adverse events:
Adverse events should be reported to the Vifor Pharma group.
safety@viforpharma.com
This is me, continue![]()
This is me, continue![]()
I am practicing from:

Austria

Austria

Belgium

Germany

Ireland

Italy

Netherlands

Portugal

Spain

Switzerland
Other
I am residing in:
Austria
Austria
Belgium
Germany
Ireland
Italy
Netherlands
Portugal
Spain
Switzerland
Other
Bitte verwenden Sie als Benutzernamen die E-Mail Adresse, welche Sie bei der Registration angegeben hatten. Falls Sie das Passwort vergessen haben, können Sie sich einen Reaktivierungslink zustellen lassen. Alternativ ist für bereits registrierte Health Professionals auch eine Anmeldung mit der HPC-Card von FMH oder pharmaSuisse möglich.
Adverse events should be reported to the Vifor Pharma group.
safety@viforpharma.com
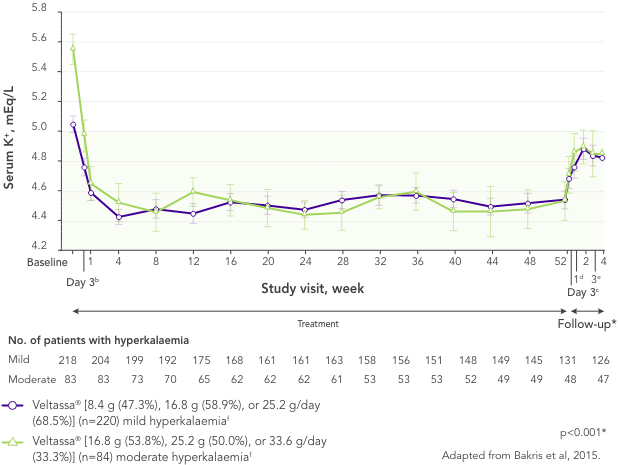
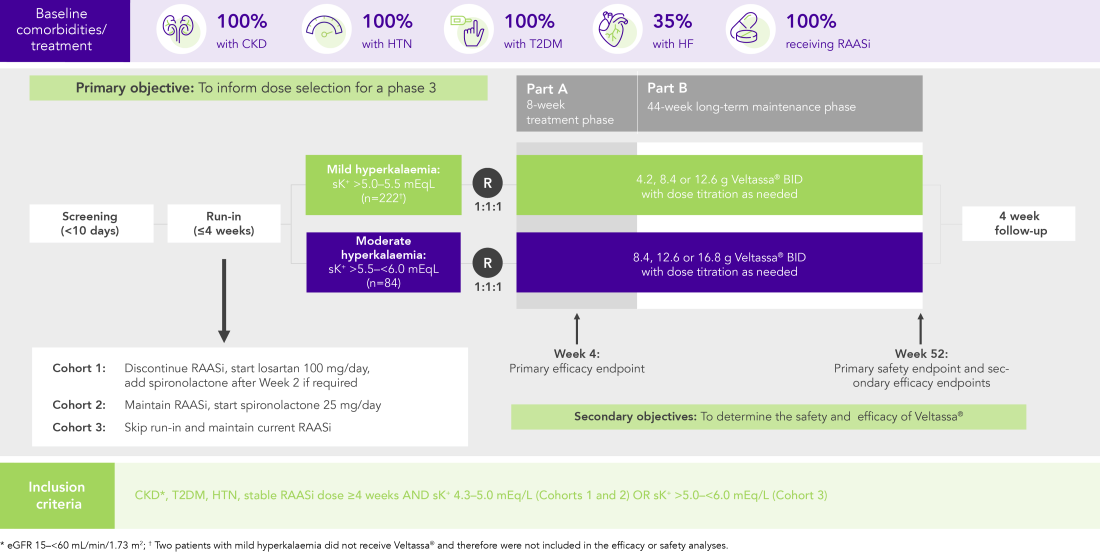
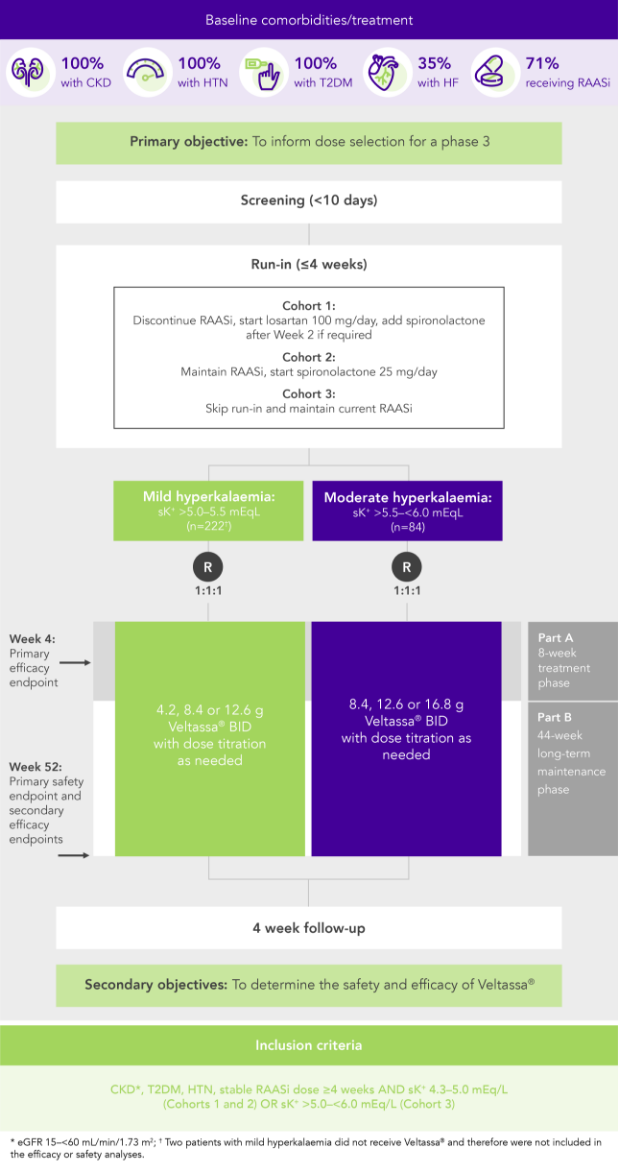
In 306 patients with T2DM, CKD, and HTN, treated with RAASi, significant decreases in serum K+ were observed after 4 weeks with Veltassa® and maintained for 1 year1 in:
![]()
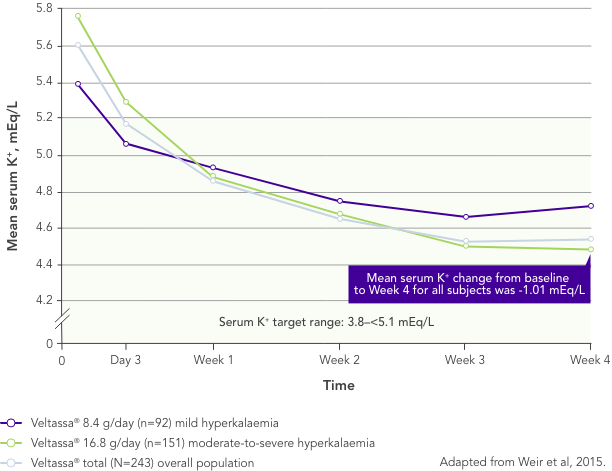
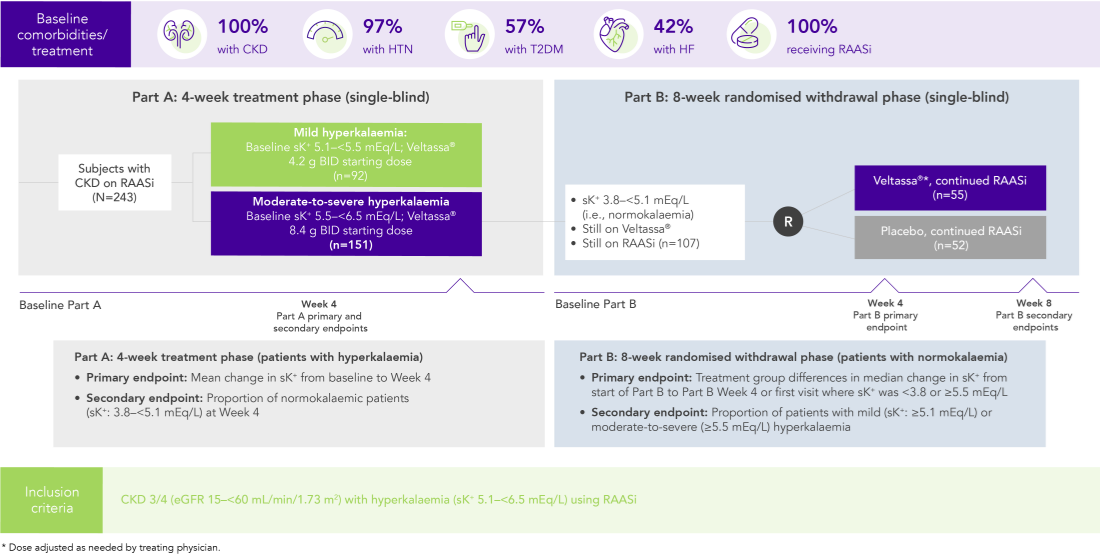
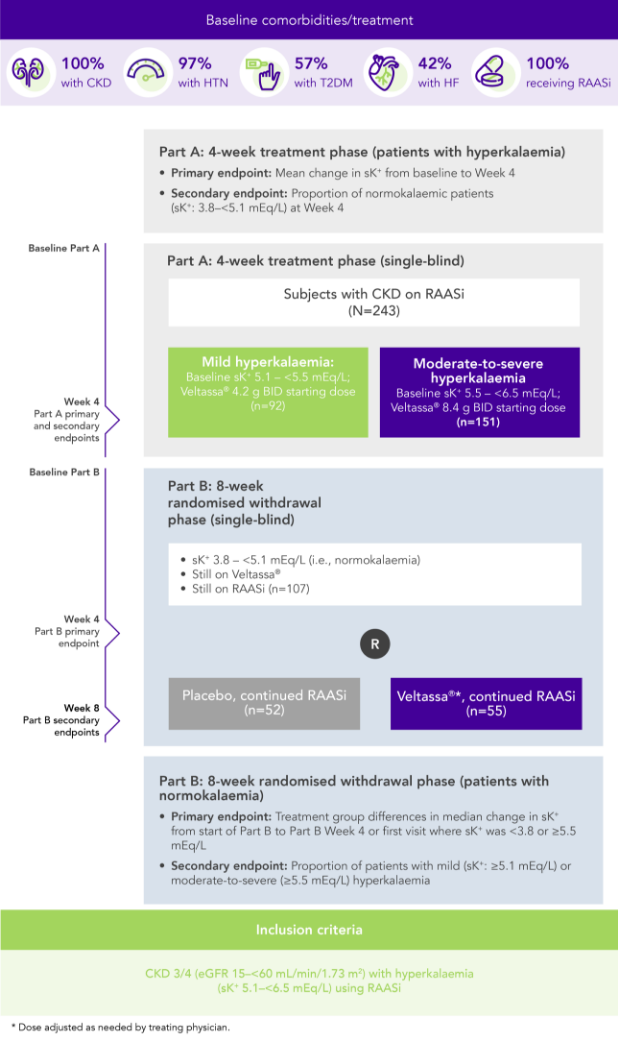
Among 243 patients with CKD and hyperkalaemia receiving RAASi, 76% had serum K+ in the target range (3.8–<5.1 mEq/L) at Week 42
Similar results in patients with:
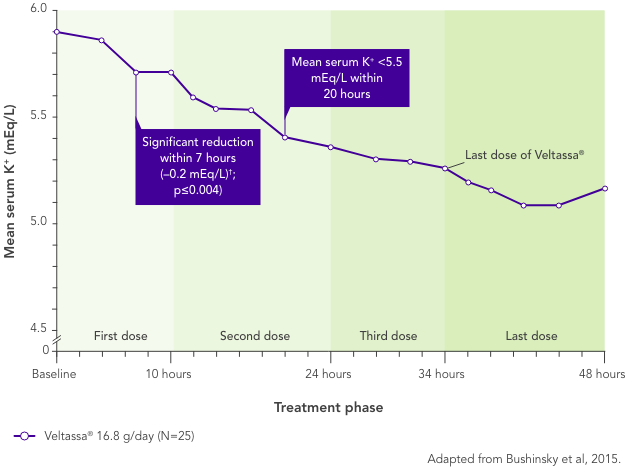
In patients with CKD and hyperkalaemia on RAASi, Veltassa® resulted in serum K+ reductions 4–7 hours after the first dose,3 with mean baseline serum K+ reduced at all subsequent times through 48 hours
Serum K+ did not increase before the next dose or for 24 hours after the last dose3
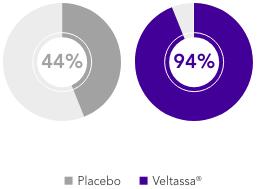
OPAL (N=243)2
100% RAASi; 42% HF; 100% CKD; 97% HTN; 57% T2DM
Proportion of patients receiving any RAASi dose at Week 8 of the randomised withdrawal phase
(exploratory endpoint)
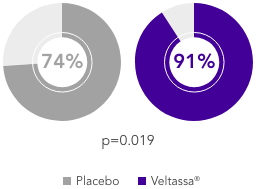
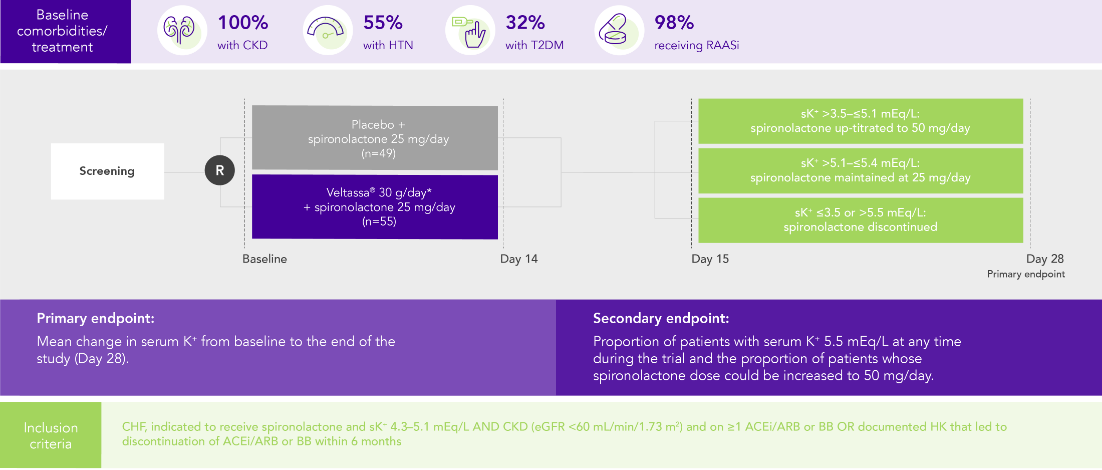
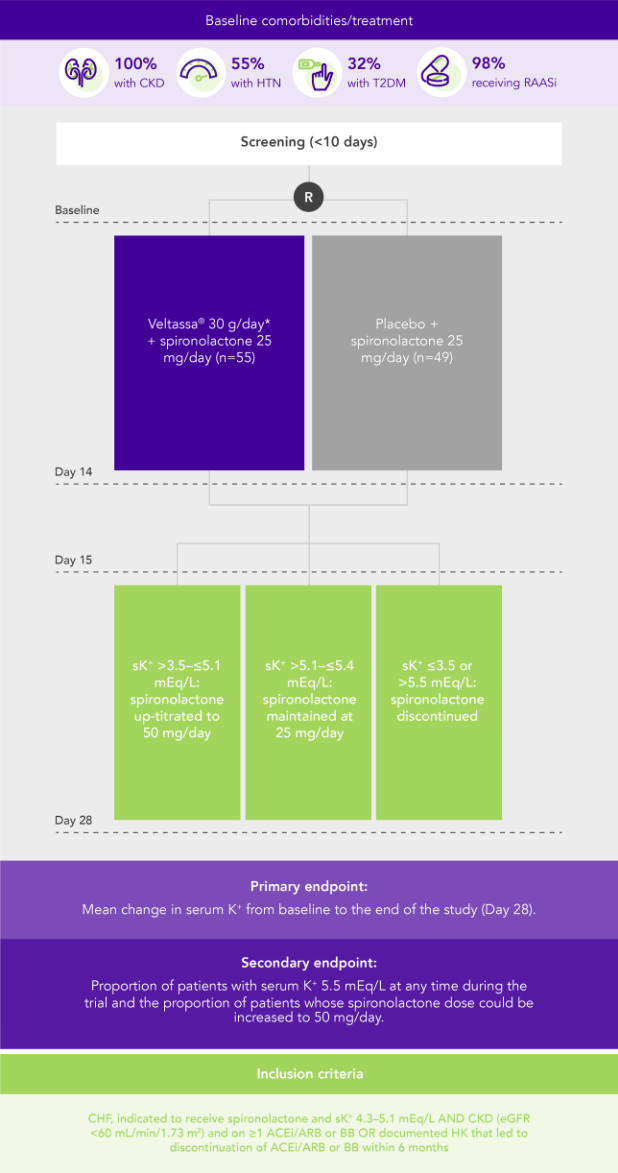
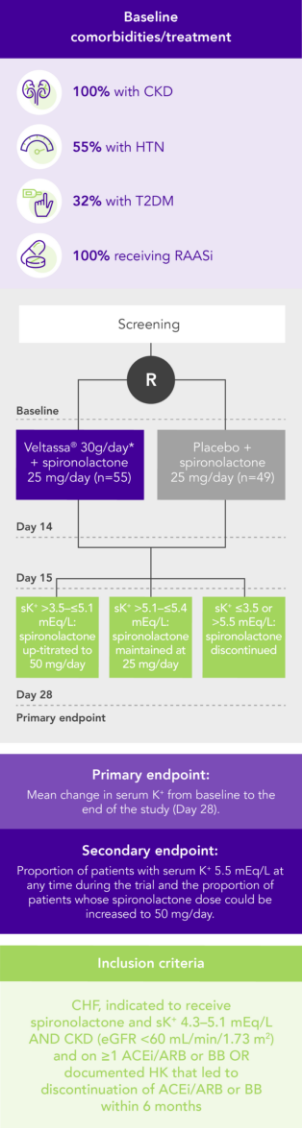
PEARL-HF (N=105)4
100% HF; 57% CKD; 32% T2DM; 98% RAASi
Proportion of patients up-titrated to spironolactone 50 mg/day
(secondary endpoint)
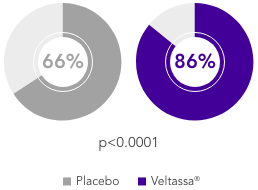
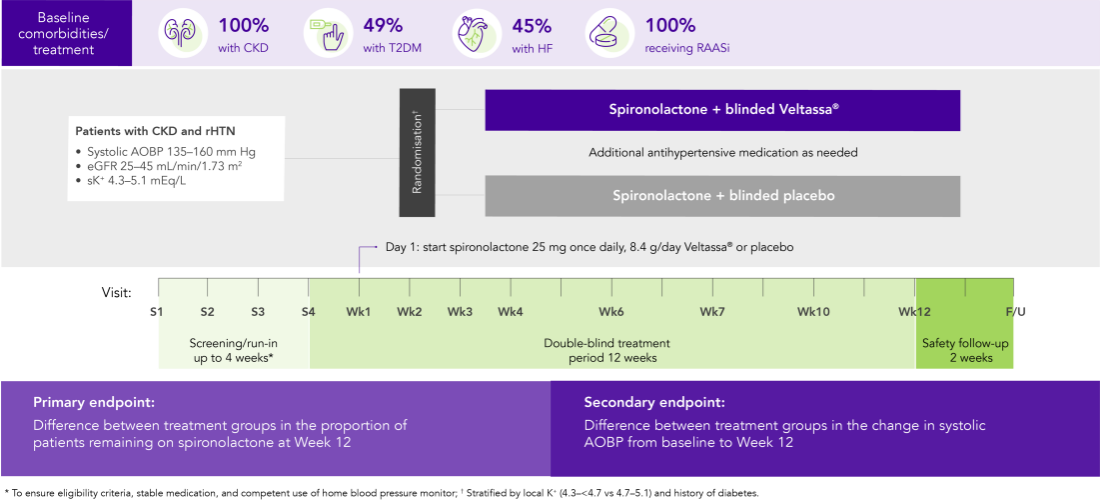
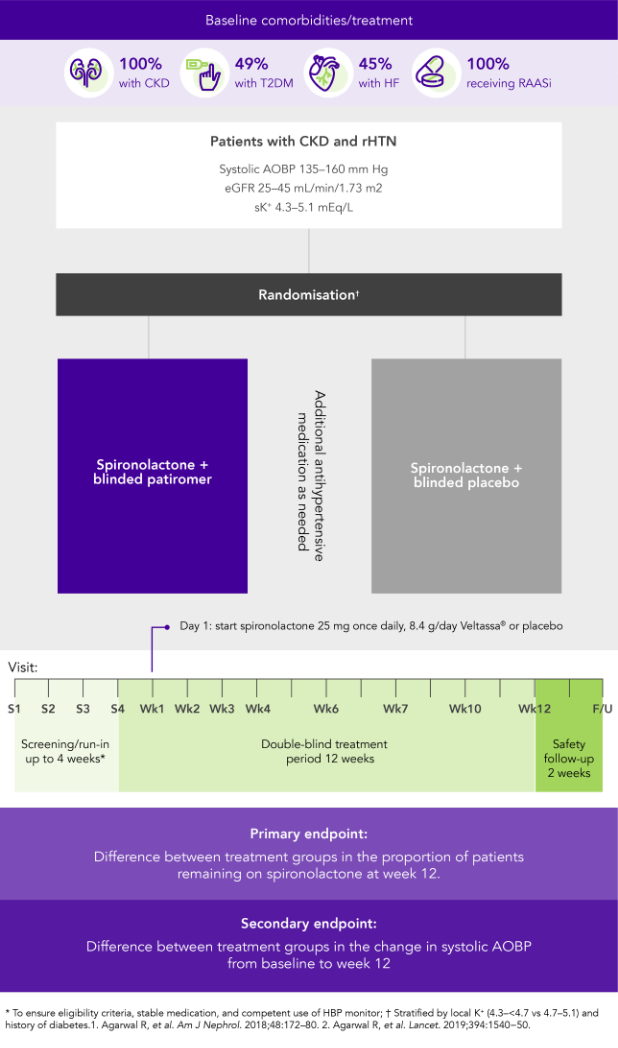
AMBER (N=295)5
100% CKD; 45% HF; 49% T2DM; 100% RAASi
Proportion of patients remaining on spironolactone at Week 12
(primary endpoint)
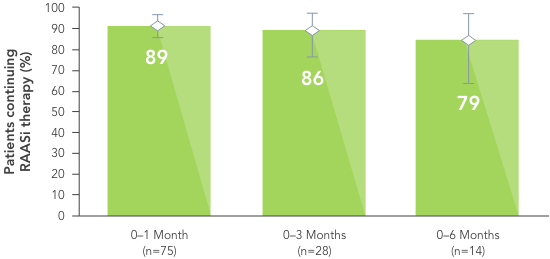
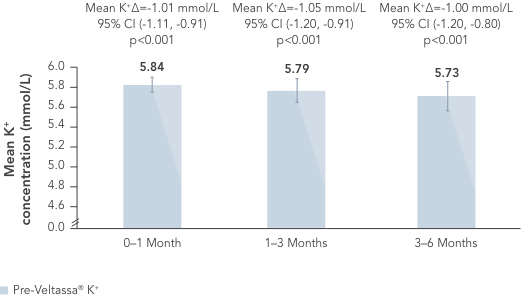
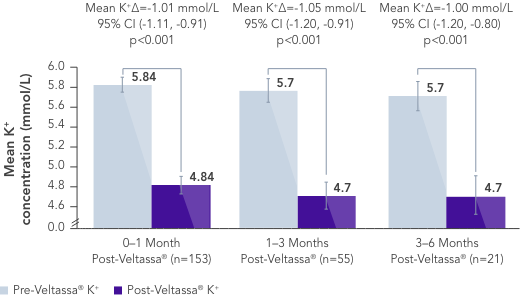
In a retrospective observational study with 288 hyperkalaemic patients with HF, T2DM or CKD, Veltassa® decreased serum K+ by an average of -1.0 mEq/L vs before treatment (p<0.001).6
In the same study, RAASi therapy was continued in ~80% of patients for 6 months.6
Similarly, in a large US healthcare database including patients with hyperkalaemia, more patients receiving Veltassa® continued RAASi therapy vs those receiving a different serum K+ binder (SPS) or no serum K+ binder.7
Treatment with Veltassa® was also associated with fewer hospital admissions and emergency department visits.7
![]()
![]()
ADRs IN CLINICAL STUDIES
| System Organ Class | Common | Uncommon |
|---|---|---|
Metabolism and nutrition disorders |
Hypomagnesaemia: 5.3% |
|
Gastrointestinal disorders |
Constipation: 6.2% Diarrhoea: 3% Abdominal pain: 2.9% Flatulence: 1.8% |
Nausea Vomiting |
![]()
![]()
The favourable safety profile observed in clinical trials is supported by evidence from real-world studies.
Concomitant administration of Veltassa® showed reduced bioavailability of only 3 drugs:8
No interaction was found with administration of oral drugs at least 3 hours apart from Veltassa®. Quinidine showed a potential drug interaction in vitro. As a precautionary measure, administration of Veltassa® should therefore be separated by at least 3 hours from other oral medicinal products.8
![]()
![]()
99.4%
receiving RAASi
at baseline
![]()
72.8%
had diabetes
![]()
81.2%
had CKD with eGFR
<60 mL/min/1.73 m2
![]()
48.7%
had HF



ACEi, angiotensin converting enzyme inhibitor; ADR, adverse drug reaction; AE, adverse event; AOBP, automated office blood pressure; ARB, angiotensin II receptor blocker; BB, beta blocker; BID, twice daily; Ca2+, calcium ions; CHF, congestive heart failure; CI, confidence interval; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GI, gastrointestinal; HF, heart failure; HK, hyperkalaemia; HTN, hypertension; K+, potassium ions; mEqL, milliequivalents per litre; RAASi, renin‐angiotensin‐aldosterone system inhibitors; rHTN, resistant hypertension; sK+, serum potassium; SPS, sodium polystyrene sulfonate; T2DM, type 2 diabetes mellitus; US, United States
aLeast squares mean (95% CI) serum potassium levels over 52 weeks and during post-treatment follow-up in patients with mild or moderate hyperkalaemia (post-hoc mixed-effects models for repeated-measures analysis).1
bAt treatment day 3, there were 202 patients with mild hyperkalaemia and 82 with moderate hyperkalaemia.
cAt follow-up day 3, there were 163 patients with mild hyperkalaemia and 58 with moderate hyperkalaemia.
dAt follow-up week 1, there were 154 patients with mild hyperkalaemia and 57 with moderate hyperkalaemia.
eAt follow-up week 3, there were 126 patients with mild hyperkalaemia and 48 with moderate hyperkalaemia.
fThe recommended starting dose of Veltassa® is 8.4 g once-daily. The daily dose may be increased or decreased by 8.4 g as necessary to reach the desired target range, up to a maximum dose of 25.2 g daily.8
1. Bakris GL, et al. JAMA 2015;314(2):151−61. 2. Weir MR, et al. N Engl J Med 2015;372(3):211−21. 3. Bushinsky DA, et al. Kidney Int 2015;88(6):1427−33. 4. Pitt B, et al. Eur Heart J 2011;32(7):820−8. 5. Agarwal R, et al. Lancet 2019;394(10208):1540−50. 6. Kovesdy CP, et al. Postgrad Med 2020;132:176–83. 7. Desai NR, et al. PLoS One 2020 Jan 7;15(1):e0226844. doi: 10.1371/journal.pone.0226844. 8. Veltassa® SmPC. 9. Li L, et al. J Cardiovasc Pharmacol Ther 2016;21(5):456−65. 10. Data on file, Relypsa Inc. 11. Pitt B, et al. ESC Heart Fail 2018;5(4):592−602. 12. Seferovic PM, et al. Eur J Heart Fail 2019;21:1169–86. 13. KDIGO Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease Kidney Int 2020;98(Suppl 4S):S1–S116.
VELTASSA es un medicamento de venta con receta que se utiliza para tratar los niveles elevados de potasio en la sangre (hiperpotasemia). Está aprobado para su uso en adultos y pacientes pediátricos de 12 años en adelante.
No tome VELTASSA si usted es alérgico a VELTASSA o a cualquiera de sus ingredientes.
Antes de tomar VELTASSA, informe a su médico sobre todas sus condiciones médicas, incluyendo si usted:
Conozca los medicamentos que toma. Arme una lista de ellos para mostrársela a su médico y farmacéutico cuando obtenga un nuevo medicament. Infórmele al médico sobre todos los medicamentos que toma, incluyendo los medicamentos recetados y de venta libre, las vitaminas y los suplementos a base de hierbas.
VELTASSA puede causar efectos secundarios graves, que incluyen los siguientes:
Los siguientes efectos secundarios de VELTASSA son los más frecuentes en pacientes adultos: estreñimiento, niveles bajos de magnesio, diarrea, náuseas, molestias en la zona del estómago (abdominales) y gases. En un estudio con pacientes pediátricos, el perfil de seguridad de VELTASSA resultó similar al de los adultos.
Infórmele a su médico si tiene algún efecto secundario que le moleste o que no desaparezca. Estos no son todos los efectos secundarios posibles de VELTASSA. Puede informar de los efectos secundarios a la FDA llamando al 1-800-FDA-1088 o en www.fda.gov/medwatch.
La información de riesgo proporcionada aquí no es exhaustiva y no reemplaza la consulta con su médico sobre su afección médica o tratamiento. Para obtener más información sobre VELTASSA, hable con su proveedor de atención médica o farmacéutico. Haga clic aquí para consultar la información de prescripción completa.
VELTASSA es un medicamento de venta con receta que se utiliza para tratar los niveles elevados de potasio en la sangre (hiperpotasemia). Está aprobado para su uso en adultos y pacientes pediátricos de 12 años en adelante.
No tome VELTASSA si usted es alérgico a VELTASSA o a cualquiera de sus ingredientes.
Antes de tomar VELTASSA, informe a su médico sobre todas sus condiciones médicas, incluyendo si usted:
Conozca los medicamentos que toma. Arme una lista de ellos para mostrársela a su médico y farmacéutico cuando obtenga un nuevo medicament. Infórmele al médico sobre todos los medicamentos que toma, incluyendo los medicamentos recetados y de venta libre, las vitaminas y los suplementos a base de hierbas.
VELTASSA puede causar efectos secundarios graves, que incluyen los siguientes:
Los siguientes efectos secundarios de VELTASSA son los más frecuentes en pacientes adultos: estreñimiento, niveles bajos de magnesio, diarrea, náuseas, molestias en la zona del estómago (abdominales) y gases. En un estudio con pacientes pediátricos, el perfil de seguridad de VELTASSA resultó similar al de los adultos.
Infórmele a su médico si tiene algún efecto secundario que le moleste o que no desaparezca. Estos no son todos los efectos secundarios posibles de VELTASSA. Puede informar de los efectos secundarios a la FDA llamando al 1-800-FDA-1088 o en www.fda.gov/medwatch.
La información de riesgo proporcionada aquí no es exhaustiva y no reemplaza la consulta con su médico sobre su afección médica o tratamiento. Para obtener más información sobre VELTASSA, hable con su proveedor de atención médica o farmacéutico. Haga clic aquí para consultar la información de prescripción completa.